Vaccine Effectiveness Hits as Low as Minus-66% in the Over-40s, New PHE Data Shows
View attachment 231964
The new Public Health England (PHE)
Vaccine Surveillance report was released on Thursday, allowing us to update our
estimates of unadjusted vaccine effectiveness from real-world data.
Oddly, the report appeared on a new webpage this week, but the
old page didn’t include a note to let you know, so it took me a while to discover it had appeared and where it was.
Following last week’s ‘
fact check‘ from Full Fatuous – ostensibly of my piece but with some words of admonition for PHE as well, particularly over the accuracy of the population data – a new note appeared in the report: “Interpretation of the case rates in vaccinated and unvaccinated population is particularly susceptible to changes in denominators and should be interpreted with extra caution.” So there you go. All estimates in this post are based on the data PHE uses and are valid insofar as that data is accurate.
As before, the data is just for a four-week period, which, given that the early part of the Delta surge was dominated by the unvaccinated and the latter part has seen infections rise in the vaccinated, seems to me a mistake. A fairer view would cover the whole Delta surge (as with the
estimates I make from the data in the Technical Briefings), but in any case the report gives a snapshot of current relative infection rates.
As Full Fatuous pointed out, PHE don’t recommend using this data to estimate vaccine effectiveness, saying it’s “not the most appropriate method” because it’s unadjusted for risk factors (and, inevitably, they don’t provide the data you’d need to adjust it). However, even if not recommended by PHE, it is certainly a valid method of calculating vaccine effectiveness, which is just a figure which states the relative risk reduction in the vaccinated group, as long as you bear in mind its limitations. All vaccine effectiveness estimates have limitations, and while adjusting for confounding factors is in principle important, it is helpful only if done well, and
manystudies do not do it well. Unadjusted estimates from raw data are a necessary starting point.
Perhaps the key confounder for the estimates of vaccine effectiveness against infection given here is whether people have been previously infected, with a common assumption being that a higher proportion of the unvaccinated will be previously infected, due to it being a potential factor in people’s decision not to be vaccinated. This may well artificially lower the vaccine effectiveness estimates, but since no one has yet produced data showing how antibodies-from-infection split between vaccinated and unvaccinated it is hard to know how far this is the case.
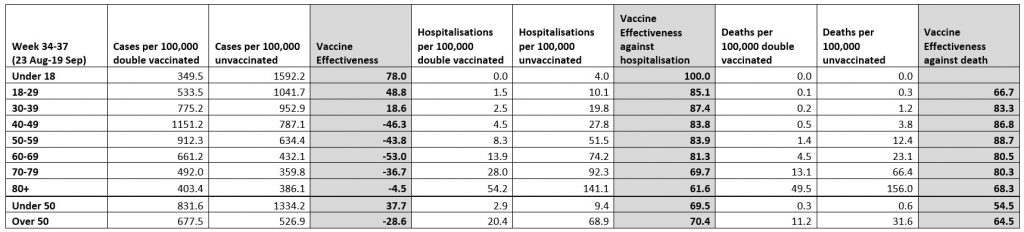
Unvaccinated here means actually unvaccinated, not partially vaccinated or post-jab. Hospitalisation means “cases presenting to emergency care (within 28 days of a positive specimen) resulting in an overnight inpatient admission”.
View attachment 231965
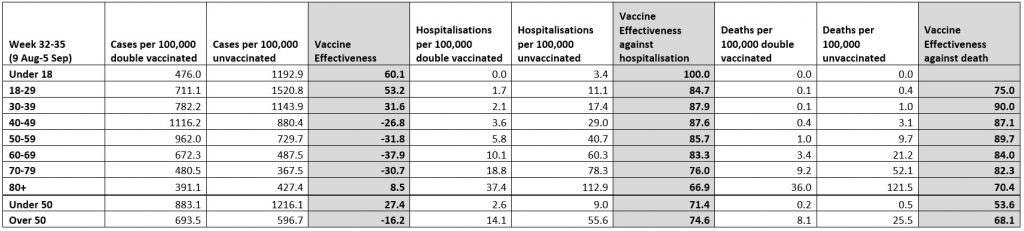
As England’s drawn-out Delta outbreak drags on, the infection rates in the vaccinated continue to outpace those in the unvaccinated, reducing (unadjusted) vaccine effectiveness further. For the 60s age group, infection rates are 63% higher in the vaccinated than in the unvaccinated, up from 53% last week, giving an (unadjusted) vaccine effectiveness of minus-63%. But that has been topped this week by the 40s age group, the vaccinated among whom now have an infection rate no less than 66% higher than the unvaccinated, up from 46% in last week’s report and 27% in the report for the month ending September 5th. Vaccine effectiveness has been heading downward in the 30s age group as well, now just 8%, though interestingly it has actually been increasing in the under-18s. On this data, vaccine protection against serious illness and death appears to be holding up. I have included the two previous tables below for comparison.
With infection rates now, on this data, much higher in the vaccinated than the unvaccinated, what remaining justification can there be for vaccine passports, vaccine mandates, and any other policy based on the assumption that vaccines protect other people? When will the Government face up to the reality that vaccines provide poor protection against infection, poor protection against transmission, and thus poor protection of others, and so there is no justification for continuing to build up the infrastructure of a two-tier, discriminatory state
 1
1






")

